
Pathology
The initial injury occurs from an acute valgus force to the ligament or from repetitive stress from stretching this ligament. The acute injury most commonly occurs simultaneously with an elbow dislocation. A common mechanism causing elbow dislocations includes falling on an outstretched hand combined with a twisting motion. The most common form of this chronic injury is from throwing.
Surgical Techniques
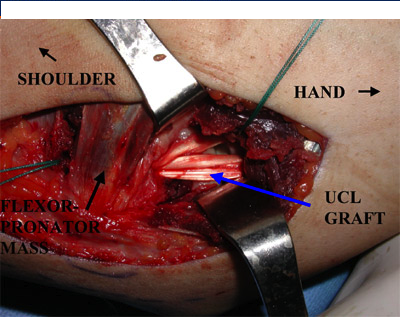
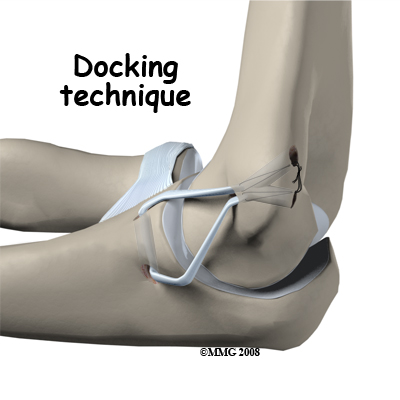
Grade III sprains of the ulnar collateral ligament requires reconstructive surgery of the anterior bundle for complete recovery. This surgery consists of replacing the bundle with a tendon from another area of the body, most commonly from the distal palmaris longus of the wrist or the extensor hallucis if the patient doesn’t posses a palmaris longus. The most common and efficient resulting technique to substitute the ligament is called the docking technique. A 2006 study on the docking technique revealed a 92% success rate for elite baseball players returning to a pre-injury level of competition with a mean return time of 11.5 months. This technique consists of drilling two holes in the ulna and three holes in the medial epicondyle of the humerus. The autograft is then sutured on the posterior portion of the epicondyle and threaded through the two holes of the ulna, just inferior to the coronoid process. The graft is then looped back through the inferior hole of the medial epicondyle where it meets with the other end of the graft. The two ends are sutured together on the posterior portion of the epicondyle. The wrist flexors are released from their origin on the medial epicondyle or are split around the site. This intervention of the flexor digitorum superficialis, flexor carpi radialis, flexor carpi ulnaris, and palmaris longus causes soreness of the musculature but will heal completely during the immobilization phase.
The initial injury occurs from an acute valgus force to the ligament or from repetitive stress from stretching this ligament. The acute injury most commonly occurs simultaneously with an elbow dislocation. A common mechanism causing elbow dislocations includes falling on an outstretched hand combined with a twisting motion. The most common form of this chronic injury is from throwing.
Surgical Techniques
Grade III sprains of the ulnar collateral ligament requires reconstructive surgery of the anterior bundle for complete recovery. This surgery consists of replacing the bundle with a tendon from another area of the body, most commonly from the distal palmaris longus of the wrist or the extensor hallucis if the patient doesn’t posses a palmaris longus. The most common and efficient resulting technique to substitute the ligament is called the docking technique. A 2006 study on the docking technique revealed a 92% success rate for elite baseball players returning to a pre-injury level of competition with a mean return time of 11.5 months. This technique consists of drilling two holes in the ulna and three holes in the medial epicondyle of the humerus. The autograft is then sutured on the posterior portion of the epicondyle and threaded through the two holes of the ulna, just inferior to the coronoid process. The graft is then looped back through the inferior hole of the medial epicondyle where it meets with the other end of the graft. The two ends are sutured together on the posterior portion of the epicondyle. The wrist flexors are released from their origin on the medial epicondyle or are split around the site. This intervention of the flexor digitorum superficialis, flexor carpi radialis, flexor carpi ulnaris, and palmaris longus causes soreness of the musculature but will heal completely during the immobilization phase.
